Overview
Adult acquired flatfoot deformity (AAFD or AAF) is a progressive, symptomatic deformity resulting from gradual stretch of the posterior tibial tendon as well as other ligaments supporting the arch of the foot. AAFD develops after skeletal maturity, May also be referred to as posterior tibial tendon dysfunction (PTTD), although due to the complexity of the disorder AAFD is more appropriate. Significant ligamentous rupture occurs as the deformity progresses. Involved ligaments include the spring ligament, the superficial deltoid ligament, the plantar fascia, and the long and short plantar ligaments. Unilateral AAFD is more common than bilateral AAFD.
Causes
Many health conditions can create a painful flatfoot, an injury to the ligaments in the foot can cause the joints to fall out of alignment. The ligaments support the bones and prevent them from moving. If the ligaments are torn, the foot will become flat and painful. This more commonly occurs in the middle of the foot (Lisfranc injury), but can also occur in the back of the foot. In addition to ligament injuries, fractures and dislocations of the bones in the midfoot can also lead to a flatfoot deformity.
Symptoms
Symptoms are minor and may go unnoticed, Pain dominates, rather than deformity. Minor swelling may be visible along the course of the tendon. Pain and swelling along the course of the tendon. Visible decrease in arch height. Aduction of the forefoot on rearfoot. Subluxed tali and navicular joints. Deformation at this point is still flexible. Considerable deformity and weakness. Significant pain. Arthritic changes in the tarsal joints. Deformation at this point is rigid.
Diagnosis
Although you can do the "wet test" at home, a thorough examination by a doctor will be needed to identify why the flatfoot developed. Possible causes include a congenital abnormality, a bone fracture or dislocation, a torn or stretched tendon, arthritis or neurologic weakness. For example, an inability to rise up on your toes while standing on the affected foot may indicate damage to the posterior tibial tendon (PTT), which supports the heel and forms the arch. If "too many toes" show on the outside of your foot when the doctor views you from the rear, your shinbone (tibia) may be sliding off the anklebone (talus), another indicator of damage to the PTT. Be sure to wear your regular shoes to the examination. An irregular wear pattern on the bottom of the shoe is another indicator of acquired adult flatfoot. Your physician may request X-rays to see how the bones of your feet are aligned. Muscle and tendon strength are tested by asking you to move the foot while the doctor holds it.
Non surgical Treatment
Orthoses (insoles, functional orthoses, ankle supports, braces, ankle foot orthoses (AFOs)) - are usually custom-made to increase the functional stability of the foot and improve the mechanical properties of the tendon as well as reducing the actual degree of strain on the tendon. This reduces pain and inflammation. Physiotherapy - exercises and physiotherapy are often used to increase mobility, strengthen the tendon itself, stretch your Achilles tendon as well as reduce pain. Once the tendon has been stretched (stage one), the heel starts rolling outwards. Total immobilisation in a cast may help the symptoms to subside and prevent progression of the deformity in a smaller percentage of patients. Long-term use of orthoses may help stop progression of the deformity and reduce pain without surgery. Non-surgical treatment is unlikely to prevent progression to stage three and four but may be chosen by some patients who either are unsuitable for surgery or prefer not to have surgery.

Surgical Treatment
Many operations are available for the treatment of dysfunction of the posterior tibial tendon after a thorough program of non-operative treatment has failed. The type of operation that is selected is determined by the age, weight, and level of activity of the patient as well as the extent of the deformity. The clinical stages outlined previously are a useful guide to operative care (Table I). In general, the clinician should perform the least invasive procedure that will decrease pain and improve function. One should consider the effects of each procedure, particularly those of arthrodesis, on the function of the rest of the foot and ankle.
Adult acquired flatfoot deformity (AAFD or AAF) is a progressive, symptomatic deformity resulting from gradual stretch of the posterior tibial tendon as well as other ligaments supporting the arch of the foot. AAFD develops after skeletal maturity, May also be referred to as posterior tibial tendon dysfunction (PTTD), although due to the complexity of the disorder AAFD is more appropriate. Significant ligamentous rupture occurs as the deformity progresses. Involved ligaments include the spring ligament, the superficial deltoid ligament, the plantar fascia, and the long and short plantar ligaments. Unilateral AAFD is more common than bilateral AAFD.
Causes
Many health conditions can create a painful flatfoot, an injury to the ligaments in the foot can cause the joints to fall out of alignment. The ligaments support the bones and prevent them from moving. If the ligaments are torn, the foot will become flat and painful. This more commonly occurs in the middle of the foot (Lisfranc injury), but can also occur in the back of the foot. In addition to ligament injuries, fractures and dislocations of the bones in the midfoot can also lead to a flatfoot deformity.
Symptoms
Symptoms are minor and may go unnoticed, Pain dominates, rather than deformity. Minor swelling may be visible along the course of the tendon. Pain and swelling along the course of the tendon. Visible decrease in arch height. Aduction of the forefoot on rearfoot. Subluxed tali and navicular joints. Deformation at this point is still flexible. Considerable deformity and weakness. Significant pain. Arthritic changes in the tarsal joints. Deformation at this point is rigid.
Diagnosis
Although you can do the "wet test" at home, a thorough examination by a doctor will be needed to identify why the flatfoot developed. Possible causes include a congenital abnormality, a bone fracture or dislocation, a torn or stretched tendon, arthritis or neurologic weakness. For example, an inability to rise up on your toes while standing on the affected foot may indicate damage to the posterior tibial tendon (PTT), which supports the heel and forms the arch. If "too many toes" show on the outside of your foot when the doctor views you from the rear, your shinbone (tibia) may be sliding off the anklebone (talus), another indicator of damage to the PTT. Be sure to wear your regular shoes to the examination. An irregular wear pattern on the bottom of the shoe is another indicator of acquired adult flatfoot. Your physician may request X-rays to see how the bones of your feet are aligned. Muscle and tendon strength are tested by asking you to move the foot while the doctor holds it.
Non surgical Treatment
Orthoses (insoles, functional orthoses, ankle supports, braces, ankle foot orthoses (AFOs)) - are usually custom-made to increase the functional stability of the foot and improve the mechanical properties of the tendon as well as reducing the actual degree of strain on the tendon. This reduces pain and inflammation. Physiotherapy - exercises and physiotherapy are often used to increase mobility, strengthen the tendon itself, stretch your Achilles tendon as well as reduce pain. Once the tendon has been stretched (stage one), the heel starts rolling outwards. Total immobilisation in a cast may help the symptoms to subside and prevent progression of the deformity in a smaller percentage of patients. Long-term use of orthoses may help stop progression of the deformity and reduce pain without surgery. Non-surgical treatment is unlikely to prevent progression to stage three and four but may be chosen by some patients who either are unsuitable for surgery or prefer not to have surgery.
Surgical Treatment
Many operations are available for the treatment of dysfunction of the posterior tibial tendon after a thorough program of non-operative treatment has failed. The type of operation that is selected is determined by the age, weight, and level of activity of the patient as well as the extent of the deformity. The clinical stages outlined previously are a useful guide to operative care (Table I). In general, the clinician should perform the least invasive procedure that will decrease pain and improve function. One should consider the effects of each procedure, particularly those of arthrodesis, on the function of the rest of the foot and ankle.
 Achilles tendinitis is when the tendon that connects the back of your leg to your heel becomes swollen and painful near the bottom of the foot. This tendon is called the Achilles tendon. It is used for walking, running, and jumping.
Achilles tendinitis is when the tendon that connects the back of your leg to your heel becomes swollen and painful near the bottom of the foot. This tendon is called the Achilles tendon. It is used for walking, running, and jumping.






 Basically a man should be aware of the same requirements for a proper fit as stated above. T he shoe should always be fitted for comfort and not for the size you think you wear. When fitting a shoe, late afternoon is the best time because your feet may be slightly larger. T hey should also be fitted in a standing position to make sure that the weight bearing is accommodated in the size of the shoe. Some individuals will find that an orthotic support will be of value. Follow the soak by massaging with a good analgesic balm. If the pain from the neuroma is intolerable and the conservative management has failed to help, there are surgical options. There are surgical procedures designed to remove the neuroma and the portion of the nerve that is causing pain. There is also a surgery to sever the ligament that crosses over the nerve. This technique is called nerve decompression. These procedures are performed in an out patient facility so that the patient can return home right after the surgery is finished. Following the surgery there is a chance that the neuroma may grow again. If the there is neuroma regrowth and the pain persists, additional surgery may be needed. The color used varies with the seasons, so women can feel stylish all the year round. The fall colors include the green, brown and orange while the spring and the summer collection contains the bright colors like lime green, yellow, and electric pink P90X, or Power 90 Extreme, is a industrial house exercise program, known because of its intensity.1 It is designed to take 90 days, and is made up of training program which employs cross-training (weight training, fighting styles, yoga and calisthenics) and personalization, combined with a nutrition and health supplement plan. Plantar fasciitis painis a common type of foot pain in athletes for a number of reasons. Runners tend to exercise too long and applytoo much stress to the feet and plantar fascia, and those with flatfeet can be at a higher risk. Repetitive stress on the plantar fasciacan be caused by wearing shoes that lack support and running routinesthat are too long. Inflammation occurs as the fibers tear, causingsevere pain. Although the healing process continues for up to 1 year, you should be able to return to impact type activity at around 3 months. This will depend on the type of operation you have and how you respond to surgery. A job that requires standing most of the time could lead to the feet hurting in the morning. Long hours of standing apply undue pressure on the feet, especially on the tendons and nerve endings. The constant weight the feet have to bear leads to formation of small tears in the tendons and causes the nerves to become inflamed. These conditions are enough to cause stabbing pain in the feet especially in the mornings. Any new exercise routine that requires use of feet may cause sudden foot cramps in the mornings. Running, jogging and cycling could give the feet mild to severe cramping in the morning.
Basically a man should be aware of the same requirements for a proper fit as stated above. T he shoe should always be fitted for comfort and not for the size you think you wear. When fitting a shoe, late afternoon is the best time because your feet may be slightly larger. T hey should also be fitted in a standing position to make sure that the weight bearing is accommodated in the size of the shoe. Some individuals will find that an orthotic support will be of value. Follow the soak by massaging with a good analgesic balm. If the pain from the neuroma is intolerable and the conservative management has failed to help, there are surgical options. There are surgical procedures designed to remove the neuroma and the portion of the nerve that is causing pain. There is also a surgery to sever the ligament that crosses over the nerve. This technique is called nerve decompression. These procedures are performed in an out patient facility so that the patient can return home right after the surgery is finished. Following the surgery there is a chance that the neuroma may grow again. If the there is neuroma regrowth and the pain persists, additional surgery may be needed. The color used varies with the seasons, so women can feel stylish all the year round. The fall colors include the green, brown and orange while the spring and the summer collection contains the bright colors like lime green, yellow, and electric pink P90X, or Power 90 Extreme, is a industrial house exercise program, known because of its intensity.1 It is designed to take 90 days, and is made up of training program which employs cross-training (weight training, fighting styles, yoga and calisthenics) and personalization, combined with a nutrition and health supplement plan. Plantar fasciitis painis a common type of foot pain in athletes for a number of reasons. Runners tend to exercise too long and applytoo much stress to the feet and plantar fascia, and those with flatfeet can be at a higher risk. Repetitive stress on the plantar fasciacan be caused by wearing shoes that lack support and running routinesthat are too long. Inflammation occurs as the fibers tear, causingsevere pain. Although the healing process continues for up to 1 year, you should be able to return to impact type activity at around 3 months. This will depend on the type of operation you have and how you respond to surgery. A job that requires standing most of the time could lead to the feet hurting in the morning. Long hours of standing apply undue pressure on the feet, especially on the tendons and nerve endings. The constant weight the feet have to bear leads to formation of small tears in the tendons and causes the nerves to become inflamed. These conditions are enough to cause stabbing pain in the feet especially in the mornings. Any new exercise routine that requires use of feet may cause sudden foot cramps in the mornings. Running, jogging and cycling could give the feet mild to severe cramping in the morning.  And she explained, very sincerely, in her sweet country drawl; "If I don't give them the money, they will go out and find the money some other way. They will steal it, or hurt someone to get it. They will end up in jail. I will be at fault, because none of that would have happened if I had only given them the money to begin with. If I give them what they want, I can stop other people from getting hurt. I can stop them from going to jail." Texans lineman Duane Brown will have his 78-game consecutive starts streak snapped due to a sprained toe. (Frederick Breedon/Getty Images) A hammer toe is a toe that is contracted at the PIP joint (middle joint in the toe), potentially leading to severe pressure and pain. Ligaments and tendons that have tightened cause the toe's joints to curl downwards. Hammer toes may occur in any toe except the big toe. There is often discomfort at the top part of the toe due to rubbing against the shoe. Hammer toes are classified based on the mobility of the toe joints. There are two types - flexible and rigid. In a flexible hammer toe, the joint has the ability to move. This type of hammer toe can be straightened manually. Cause. If the hooves are not properly trimmed on a regular basis, the horse is more susceptible to suffering from navicular due to abnormal growth of the hoof. The hoof grows and wears in accordance with the footing that the horse is kept on. The bone may become immobile and cause poor circulation in the hoof. In extreme conditions, the coffin bone will slowly sink to the floor of the hoof and may pierce the bottom of hoof. The condition usually occurs only in the front feet and generally affects both feet. Hammertoes are most commonly found on the second (next to the big toe) and fifth (or small) toes. Because of this abnormal toe position, the joint of the toe becomes prominent on top of the buckled toe. The tendons and ligaments then begin to contract and accelerate the problem. Skin irritation (inflamed skin areas) or even corns – (an accumulation of hard dead skin cells) may form on top of these prominent, contracted joints where shoes are likely to rub. This usually will lead to pain and inability to wear some types of shoes comfortably, especially if the pressure or corn is on the small toe.
And she explained, very sincerely, in her sweet country drawl; "If I don't give them the money, they will go out and find the money some other way. They will steal it, or hurt someone to get it. They will end up in jail. I will be at fault, because none of that would have happened if I had only given them the money to begin with. If I give them what they want, I can stop other people from getting hurt. I can stop them from going to jail." Texans lineman Duane Brown will have his 78-game consecutive starts streak snapped due to a sprained toe. (Frederick Breedon/Getty Images) A hammer toe is a toe that is contracted at the PIP joint (middle joint in the toe), potentially leading to severe pressure and pain. Ligaments and tendons that have tightened cause the toe's joints to curl downwards. Hammer toes may occur in any toe except the big toe. There is often discomfort at the top part of the toe due to rubbing against the shoe. Hammer toes are classified based on the mobility of the toe joints. There are two types - flexible and rigid. In a flexible hammer toe, the joint has the ability to move. This type of hammer toe can be straightened manually. Cause. If the hooves are not properly trimmed on a regular basis, the horse is more susceptible to suffering from navicular due to abnormal growth of the hoof. The hoof grows and wears in accordance with the footing that the horse is kept on. The bone may become immobile and cause poor circulation in the hoof. In extreme conditions, the coffin bone will slowly sink to the floor of the hoof and may pierce the bottom of hoof. The condition usually occurs only in the front feet and generally affects both feet. Hammertoes are most commonly found on the second (next to the big toe) and fifth (or small) toes. Because of this abnormal toe position, the joint of the toe becomes prominent on top of the buckled toe. The tendons and ligaments then begin to contract and accelerate the problem. Skin irritation (inflamed skin areas) or even corns – (an accumulation of hard dead skin cells) may form on top of these prominent, contracted joints where shoes are likely to rub. This usually will lead to pain and inability to wear some types of shoes comfortably, especially if the pressure or corn is on the small toe. 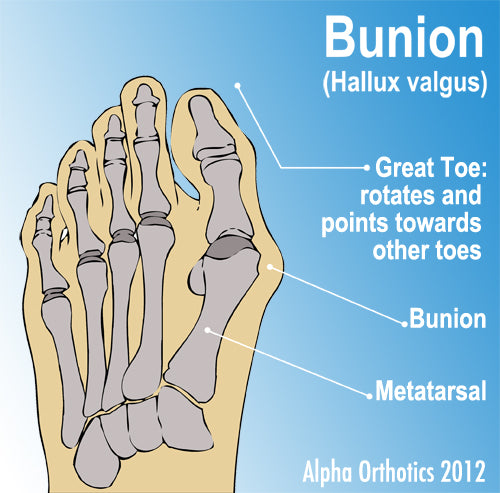 Can anyone wear a "Fit Flop"? Caution should be taken in picking any shoe. Foot type is important to evaluate. Many people with significant flexible flat feet or unstable foot type should not wear the "Fit Flop" because the destabilizing technology can actually accentuate the stress on their foot. If you require in-shoe foot orthotics, the "Fit Flop" is probably not for you. Dr Marybeth Crane is a sports medicine podiatrist and has been interviewed extensively in the last five years on the nature of flip-flop injuries. For more information on foot-related topics, visit my website at www.faant.com or my running specific website www.myrundoc.com Cavus foot is the term for a condition in which arches are abnormally high. The American College of Foot and Ankle Surgeons explains that due to the high arch, an excessive amount of weight is forced upon the ball and heel of the foot. Consequently, this causes pain when standing or walking and makes the ankle more susceptible to sprains because the foot tends to tilt inward. Cavus foot occurs at any age and happens in one or both feet. A condition referred to as plantar fasciitis also impacts the arch of the foot. This condition is an inflammation of the fibrous ligaments in the arch. Dr. McClanahan states that patients with bunion deformities respond favorably to conservative treatment methods, which include the use of a toe spacer to reposition all the toes—not just the big toe—into their natural anatomical positions. McClanahan suggests introducing range-of-motion exercises to manipulate the big toe into an adducted position (the opposite direction of the way it’s deviating) and selecting shoes with a toe box wide enough to accommodate the toe spacer or bunion splint. Getting the services of the best bunion treatment providers would eventually guarantee you with the best and timely response for your betterment. About the Author Hereditary and anatomical predisposition combined with minor injury from wearing narrow pointed shoes and high heels, uncorrected excessive pronation with resultant altered foot mechanics, added body weight, injury, arthritis and weakened intrinsic muscles are all considered important factors that contribute to the condition. The foot is painful because the bunion becomes inflamed from shoe irritation, degenerative arthritis at the first metatarsophalangeal joint or both. Here is a picture of a hallux valgus deformity compared to a normal big toe. The deformed toe is on the left, the normal big toe joint on right.
Can anyone wear a "Fit Flop"? Caution should be taken in picking any shoe. Foot type is important to evaluate. Many people with significant flexible flat feet or unstable foot type should not wear the "Fit Flop" because the destabilizing technology can actually accentuate the stress on their foot. If you require in-shoe foot orthotics, the "Fit Flop" is probably not for you. Dr Marybeth Crane is a sports medicine podiatrist and has been interviewed extensively in the last five years on the nature of flip-flop injuries. For more information on foot-related topics, visit my website at www.faant.com or my running specific website www.myrundoc.com Cavus foot is the term for a condition in which arches are abnormally high. The American College of Foot and Ankle Surgeons explains that due to the high arch, an excessive amount of weight is forced upon the ball and heel of the foot. Consequently, this causes pain when standing or walking and makes the ankle more susceptible to sprains because the foot tends to tilt inward. Cavus foot occurs at any age and happens in one or both feet. A condition referred to as plantar fasciitis also impacts the arch of the foot. This condition is an inflammation of the fibrous ligaments in the arch. Dr. McClanahan states that patients with bunion deformities respond favorably to conservative treatment methods, which include the use of a toe spacer to reposition all the toes—not just the big toe—into their natural anatomical positions. McClanahan suggests introducing range-of-motion exercises to manipulate the big toe into an adducted position (the opposite direction of the way it’s deviating) and selecting shoes with a toe box wide enough to accommodate the toe spacer or bunion splint. Getting the services of the best bunion treatment providers would eventually guarantee you with the best and timely response for your betterment. About the Author Hereditary and anatomical predisposition combined with minor injury from wearing narrow pointed shoes and high heels, uncorrected excessive pronation with resultant altered foot mechanics, added body weight, injury, arthritis and weakened intrinsic muscles are all considered important factors that contribute to the condition. The foot is painful because the bunion becomes inflamed from shoe irritation, degenerative arthritis at the first metatarsophalangeal joint or both. Here is a picture of a hallux valgus deformity compared to a normal big toe. The deformed toe is on the left, the normal big toe joint on right.  RSS Feed
RSS Feed
